Interventions via Catheter for Coronary Artery Disease
Catheter procedures are used to open coronary arteries that have been blocked or narrowed by CAD. These interventions are collectively known as Percutaneous Coronary Intervention (PCI). While patients undergoing non-emergent/scheduled PCI once stayed in hospital overnight, they are now often discharged the same day as the procedure is performed.
PCI is performed in a cardiac catheterization laboratory using fluoroscopy. Anti-platelet medications are often administered at the beginning of the procedures. An introducer is placed into the femoral, radial or brachial artery.
View this example of a PCI via the femoral artery:
While the incidence of serious complications after PCI have decreased considerably in recent years, there is still a possibility of coronary artery spasm, coronary artery dissection, renal failure induced by contrast, dysrhythmia, vasovagal response during manipulation of the sheaths and acute coronary thrombosis.
Commonly used interventions are:
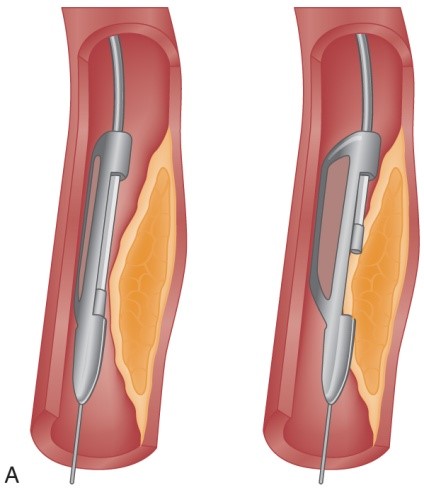
Atherectomy
The excision and removal of the atherosclerotic plaque by cutting, shaving or grinding.
Two types of catheters are used:
Directional Coronary Atherectomy (DCA)
- Rotating cup shaped blade within a windowed cylindrical chamber on one side and low-inflation balloon on the other
- Catheter is positioned in the lesion, balloon is inflated, forcing the plaque into the chamber window
- Cutting blade then used to shave the protruding plaque that is then collected into the chamber
Rotational Ablation
- Rotating cup shaped blade within a windowed cylindrical chamber on one side and low-inflation balloon on the other
- Catheter is positioned in the lesion, balloon is inflated, forcing the plaque into the chamber window
- Cutting blade then used to shave the protruding plaque that is then collected into the chamber

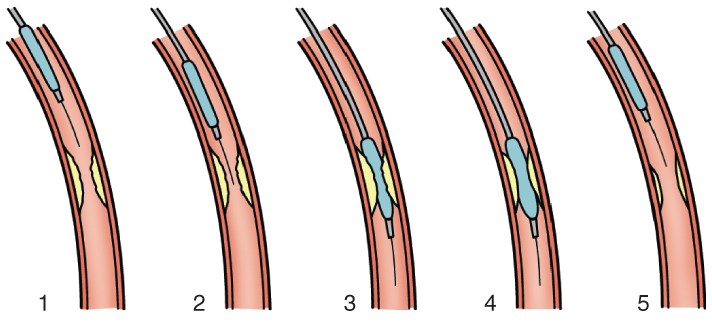
Balloon Angioplasty
- Percutaneous transluminal coronary angioplasty (PTCA) was introduced in 1977 as an alternative to surgical intervention
- Patients with single or multi-vessel disease my be candidates for PCTA
- While once impossible, it is now possible for vessels to be totally dilated
- Involves the use of a balloon-tipped catheter that, when advanced through the atherosclerotic lesion can be inflated intermittently for the purpose of dilating the stenotic area and improving blood flow
- The higher inflation pressure of the balloon stretches the wall of the coronary artery, breaks the plaque into smaller fragments and enlarges the vessel.
- When the balloon is deflated, the vessel does exert its properties of elasticity and results in 30% residual stenosis
- The procedure is considered successful if the initial stenosis is reduced to less than 50% of the vessel diameter
- The limitations of the treatment are risk of vessel occlusion and restenosis.
- PCTA is not often used in the absence of other treatment such as stent insertion
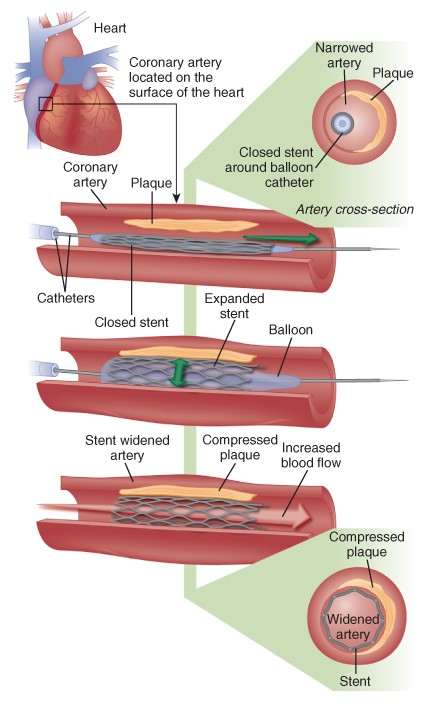
Stent Implantation
- A stent is a metal structure that is introduced into the coronary artery over a guidewire and expanded into the vessel wall at the site of the lesion
- Stents can be placed in large vessels with prominent lesions and in smaller lesions with diffuse disease, in vessels with lesions at bifurcations and vessels with thrombi
- Multiple stents may be implanted sequentially to fully cover a large area of lesion
- They comprise 90% of all interventional PCIs
They are made of many different materials and configurations to prevent restenosis, drug-eluting stents that have polymer coatings that are impregnated with medications that are slowly released at the site of placement to prevent cellular proliferation are often used.
Nursing responsibilities following a PCI procedure include care of the vascular access site, management of active closure devices if required, monitoring for any complications and providing patient education regarding post procedure care and risk factor modification.
The Cardiothoracic Learning Package produced by the Liverpool Hospital can be found here. It provides a comprehensive review of previously learned concepts and an introduction of new material regarding cardiac surgery and the care required of this patient population.